Behavioral Health Services Act (BHSA)
MHSA-to-BHSA Transformation
The Behavioral Health Services Act (BHSA) modernizes the Mental Health Services Act (MHSA), passed by voters in 2004, to address today's behavioral health system and needs.
In March 2024, voters passed Proposition 1, a transformation of California's behavioral health system. The new law includes two parts: the Behavioral Health Services Act (BHSA) and a $6.4 billion Behavioral Health Bond for community infrastructure and housing with services.
These reforms expand services to include treatment for people with substance use disorders, prioritizing care for individuals with the most serious mental illnesses, provide ongoing resources for housing interventions and workforce, and continue investments in early intervention programs. Housing is an essential component of behavioral health treatment, recovery, and stability.
Beginning July 2026, under the BHSA, 30 percent of each county's funding allocation must be used for housing interventions for Californians with the most significant behavioral health needs who are homeless or at risk of homelessness. Half of that amount is prioritized for those experiencing chronic homelessness.
Service Delivery Component Changes
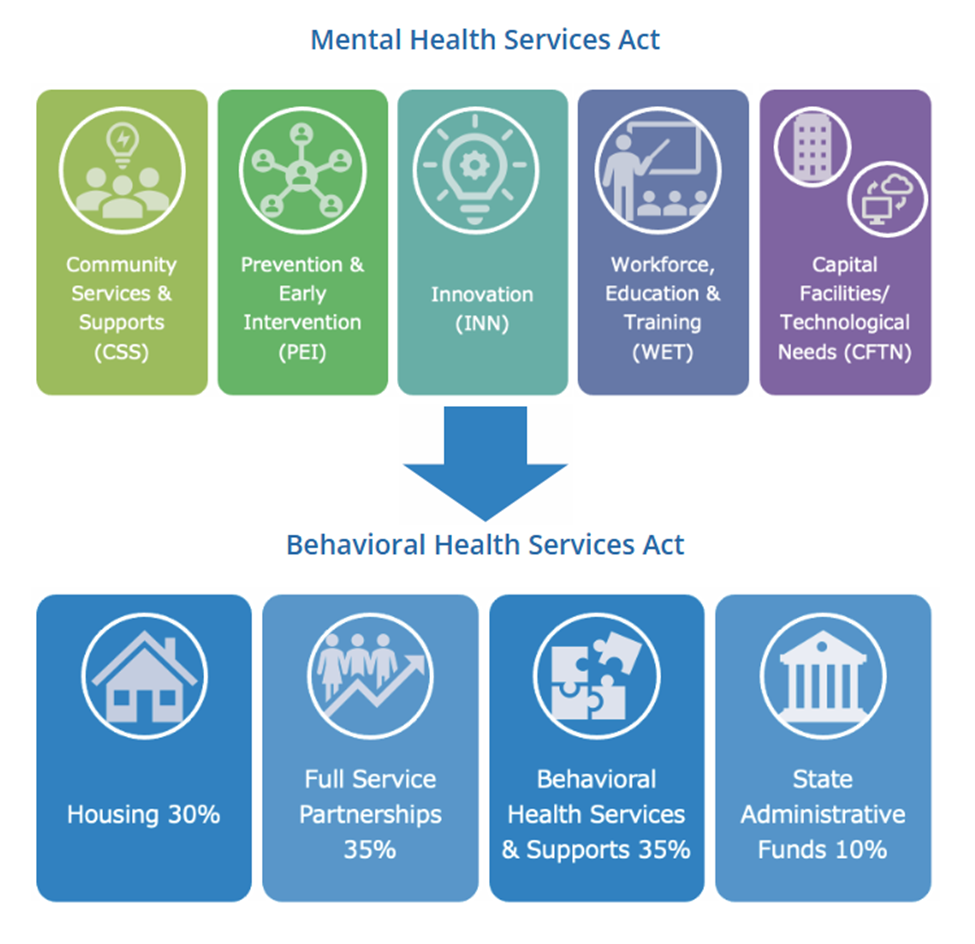
The Mental Health Services Act was designed with 5 components: Community Services and Supports (CSS), Prevention and Early Intervention (PEI), Innovation (INN), Workforce, Education, and Training (WET), & Capital Facilities and Technological Needs (CFTN) as shown below.
The new Behavioral Health Services Act will be reduced to 3 components with a 4th being statewide administration and initiatives. BHSA will continue to invest in Full-Service Partnership programs which is comprised of evidence-based practices (EBP) and a whatever-it-takes service model to treat individuals experiencing severe mental illness and substance use disorders. Behavioral Health Services & Supports (BHSS) is a component designed as a discretionary and flexible category for the County’s mandated and high-priority services.
Your Feedback is Important
Community members and participants of the Community Planning Process (CPP) may submit feedback, comment, or questions here: Behavioral Health Services Act (BHSA) Community Feedback
Below is the first of a series of informational videos discussing new statewide Behavioral Health Transformation (BHT) initiatives being implemented in SLO County.
Related Services
FAQs
-
County Integrated Plan for Behavioral Health Services and Outcomes: The Integrated Plan, the first of which a draft is due March 31, 2026, and the final due June 30, 2026, will provide a more comprehensive and transparent picture of all public local, state, and federal behavioral health funding, including Behavioral Health Services Act, Realignment, Federal Substance Abuse and Mental Health Services Administration and Projects for Assistance in Transition from Homelessness (PATH) grants, opioid settlement funds, and Medi-Cal. The plans will provide a budget of planned expenditures, reserves, and adjustments, align with state and local goals and outcome measures, and outline workforce strategies. Plans must be informed by local stakeholder input, including additional voices on the local behavioral health advisory boards.
-
County Behavioral Health Outcomes, Accountability, and Transparency Report: Counties will be required to report annually on expenditures of all local, state, and federal behavioral health funding (e.g., Behavioral Health Services Act, Realignment funding, federal Substance Abuse and Mental Health Services Administration and PATH grants, opioid settlement funds, and Medi-Cal), unspent dollars, service utilization data and outcomes with a health equity lens, workforce metrics, and other information. DHCS is authorized to impose corrective action plans on counties failing to meet certain requirements.
Performance outcomes will be developed by DHCS in consultation with counties and community input. An additional 2 percent and up to 4 percent for small counties of local Behavioral Health Services Act revenue may be used to improve planning, quality, outcomes, data reporting, and subcontractor oversight for all county behavioral health funding, on top of the existing 5 percent county planning allotment.
The Behavioral Health Services Act builds on many strategies to meet communities' needs for culturally responsive services that improve health and reduce health disparities for all, including:
-
Reducing the silos for planning and service delivery.
-
Requiring stratified data and strategies for reducing health disparities in planning, services, and outcomes.
-
Clearly advancing community-defined practices as a key strategy for reducing health disparities and increasing diverse community representation.
-
High-need individuals will benefit from the emphasis on Full Service Partnerships, which provide evidence-based programs, high-fidelity wraparound to community-defined evidence-based programs. These children and youth can benefit from a whole-person approach that is trauma-informed, age-appropriate, and in partnership with family or an individual's existing supports.
-
51 percent of early intervention funding must be directed to people 25 years of age and younger and include early childhood (0-5) mental health consultation, school-based services, and expanding early psychosis and mood disorder detection and intervention.
- Population-based programming on behavioral health and wellness to increase awareness about resources, reduce stigma, and stop behavioral health problems before they start.
- SLO County is also investing in partnering with schools in providing services through CYBHI Fee Schedule evolving historical school based services into the Student Assistance Program providing school counselors on school campuses.
The funding categories for county funding are as follows:
-
35 percent for Behavioral Health Services and Supports, including early intervention; outreach and engagement; workforce; education and training; capital facilities and technological needs; and innovative pilots and projects.
-
A majority (51 percent) of this amount must be used for intervention in the early signs of mental illness or SUDs.
-
A majority (51 percent) of early intervention services and supports must be for people 25 years of age and younger.
35 percent for Full Service Partnership programs, including comprehensive and intensive care for people at any age with the most complex needs (also known as the “whatever it takes" model).
30 percent for housing, including interventions for rental subsidies, operating subsidies, shared housing, family housing for eligible children and youth, and the non-federal share of certain transitional rent.
-
Half of this amount (50 percent) is prioritized for housing interventions for the chronically homeless.
-
Up to 25 percent may be used for capital development.
Under the Behavioral Health Services Act there are new responsibilities for state departments:
-
The California Department of Public Health (CDPH) will receive 4 percent for statewide, population-based prevention services, with 51 percent of this funding serving people 25 years of age and younger.
-
The Department of Health Care Access and Information (HCAI) will receive 3 percent for sustained statewide workforce initiatives to expand a culturally competent and well-trained behavioral health workforce.
-
DHCS, along with various state departments, will receive a portion of the remaining 3 percent (which was reduced from 5 percent) for oversight and monitoring, technical assistance, and administering programs. BHSOAC will direct the Innovation Partnership Fund, which sets aside $20 million annually to develop innovations with non-governmental partners.
-
Updates allocations for local services and state-directed funding categories.
-
Broadens the target population to include individuals with substance use disorder.
-
Focuses on the most vulnerable and at-risk groups, including children and youth.
-
Advancesevidence-based practices and community-defined practices (community-based practices that have reached a strong level of support within specific communities) as a key strategy for reducing health disparities and increasing community representation.
-
Revises county processes and improves transparency and accountability.
In addition, based on learning from previous engagement efforts, Behavioral Health Services is expanding opportunities to discuss specific topics including accessibility, care coordination and navigation, community outreach and education, crisis response services, culturally appropriate care, support for people experiencing homelessness, services for youth and transition age youth, and workforce capacity and diversity.
The allocation methodology to distribute local funding will also stay the same.
SLO BHD Services:
(800) 838-1381.
If you're seeking services for mental health and SUD services, please call us at the phone number above..
Central Coast Hotline :
1-800-783-0607
If you are having a local mental health crisis, call or text 24/7
988 Suicide and Crisis Lifeline:
988
Is available 24 hours a day, seven days a week, 365 days a year.
View more Crisis and Hotline numbers: Resource Center
